Surgery Beyond Human Hands - How Robots Are Transforming Operating Theatres

In a brightly lit operating theatre, two slender robotic arms hover over a patient’s abdomen, their movements fluid and deliberate. Each gesture is a translation of a surgeon’s intention—filtered, stabilised and refined by machinery capable of executing motions no human wrist could replicate. A few metres away, the surgeon sits not at the bedside but at a console, manipulating instruments through an immersive interface that blends vision, mechanics, and computation. This is not science fiction. This is surgery in Britain today, where robotic-assisted systems have quietly but profoundly changed the rhythm and texture of modern operative care.
Robotic surgery, once a curiosity confined to specialist centres, has become deeply embedded across the NHS. Its expansion has been driven by steadily rising demand for minimally invasive procedures, pressures on the clinical workforce, and the increasingly complex needs of an ageing population. Yet adoption has not been uniform. Nor have the clinical benefits been consistent across specialties. While enthusiasts portray robotic systems as heralding a new era of precision and safety, sceptics point to high costs, steep learning curves, and ambiguous comparative outcomes. What is clear is that robotics has begun to reshape not only how surgeons operate, but also how they train, how hospitals organise themselves, and how society thinks about the partnership between humans and machines.
A Short History of Robotic Intervention
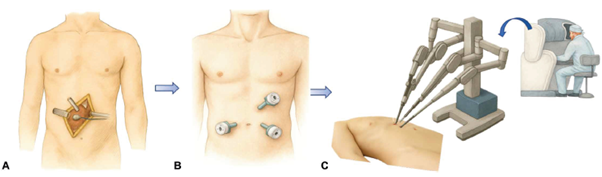
Historically surgery (A) involved interventions where internal organs were exposed with large incisions. Clinical and technical innovations in the 1980s led to the PUMA 560 (B), a repurposed industrial robot that first demonstrated how machines could position instruments with greater steadiness than even the most disciplined surgeons. It proved capable of guiding a neurosurgical biopsy needle with unprecedented accuracy, and in doing so planted the seed of a technological revolution. Through the 1990s, a wave of innovation unfolded as engineers experimented with robotic end-effectors, stereoscopic visualisation, and sophisticated teleoperation systems. It was the arrival of the da Vinci surgical system (C), launched commercially in 2000, that transformed robotics from an experimental fringe into a global industry. With its wristed instruments, three-dimensional imaging, tremor filtration, and intuitive motion scaling, da Vinci gave surgeons a degree of dexterity inside the human body that conventional laparoscopic tools simply could not match. By 2023, da Vinci systems were being used in more than 2.2 million operations annually worldwide, and the platform had become ubiquitous in urology, gynaecology, colorectal surgery and beyond.
A 2025 review in Science Robotics summarised this evolution as a steady march from mechanical augmentation toward increasing cognitive capability. As the authors noted, modern surgical robots not only restore dexterity lost in minimally invasive approaches but also offer a platform on which artificial intelligence (AI) and machine learning can be layered to support tasks ranging from tissue tracking to semi-autonomous suturing. The field, in short, has evolved from robotic arms acting as extensions of the surgeon’s hands to systems that hint at an impending future where the robot itself may assume elements of judgement and control.
What the Evidence Shows: Benefits, Trade-offs, and the Reality Behind the Hype
Much of the debate around robotic surgery hinges on whether it meaningfully improves patient outcomes. When compared with traditional open surgery, the advantages are substantial and well documented. Patients typically experience less blood loss, fewer transfusion requirements, reduced postoperative pain, shorter hospital stays and lower overall complication rates. These improvements arise from the combination of fine motor control, smaller incisions and a magnified three-dimensional perspective of the operative field.
Yet robots do not operate in a vacuum. In many specialties, the more relevant comparison is not with open surgery but with conventional laparoscopy. And here the picture becomes more complex. The Science Robotics review pointed out that, although robotic platforms offer superior ergonomics and dexterity, their superiority over laparoscopy is far less conclusive. Randomised controlled trials have repeatedly shown that complication rates, oncological outcomes, and length of stay are often similar. Operative times, by contrast, are frequently longer during early adoption, reflecting the time required to dock and configure the system, as well as the surgeon’s unfamiliarity during the learning phase.
This tension between theoretical advantages and real-world variability is a defining feature of the current era. Robots provide extraordinary consistency and reproducibility—qualities difficult for humans to match—but these benefits do not always translate into dramatic clinical differences. Instead, they manifest in more subtle patterns of predictability, standardisation and operational efficiency, features that are increasingly important to overstretched health systems.
Challenges to Rolling out Robotics in the NHS: Training the Next Generation
The NHS’s enthusiasm for robotics has outpaced its preparedness to train surgeons in their use. A 2024 national survey of UK surgical trainees found that although nearly two-thirds of NHS trusts now possess robotic platforms, only around a quarter of trainees have consistent access to simulation tools, supervised operating lists or formal curricula. Many rely on ad-hoc opportunities or personal study budgets that are already stretched thin.
The situation is reminiscent of the early years of laparoscopic surgery in the 1990s, when widespread adoption raced ahead of structured training, creating a generation of consultants who had to teach themselves on the job. But robotics raises unique challenges. Whereas basic laparoscopic skills can be acquired using relatively inexpensive box trainers, robotic systems require specialised simulators, dual-console platforms for mentoring, and coordinated team training for scrub nurses and theatre practitioners. Without this infrastructure, trainees risk graduating without adequate exposure to a technology that is rapidly becoming central to modern practice.
The Science Robotics review highlights that even teleoperated systems demand mastery of complex visuomotor skills. Surgeons must interpret three-dimensional endoscopic imagery, compensate for the lack of haptic feedback, and operate in environments where tissue deformation and occlusion can vary dramatically. For partially autonomous systems, the skill set changes again: surgeons must learn to supervise and override algorithms, interpret system uncertainties, and make meta-level decisions about when to trust or intervene.
A rare qualitative study conducted in 2025 sheds light on how surgical teams respond when a new robotic system is introduced alongside an established one. The hospital in question had long used the da Vinci system but was now adopting the Dexter robot. Surgeons initially praised the Dexter for its faster docking and the ability to switch quickly between robotic and manual modes. But when asked which system they would choose for themselves or a loved one, nearly all opted for the better-established da Vinci, citing its long track record, superior instrument articulation and unmatched familiarity among staff. Operating room nurses were more ambivalent. The introduction of the new system created disruption at first, bringing unfamiliar workflows, altered positioning routines and a heightened sense of stress during early cases. They noted that although communication improved, logistical demands increased. Anesthesiologists expressed concern about prolonged operating times during the team’s learning curve.
This shifting landscape raises urgent questions for workforce planning. If robots become integral to surgical care, national training programmes must adapt accordingly. Without intervention, the UK risks a bifurcation between surgeons proficient with robots and those effectively excluded from advanced roles.
The Next Frontier: Autonomous and AI‑Enhanced Surgery
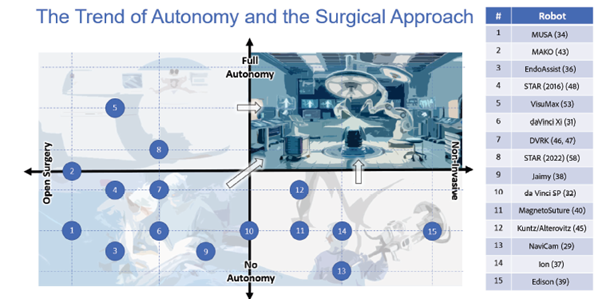
Perhaps the most provocative developments in robotics come from the integration of artificial intelligence. The Science Robotics review lays out a taxonomy of surgical autonomy, ranging from purely manual procedures (Level 0) to teleoperated assistance (Level 1), task autonomy (Level 2), supervised autonomy (Level 3), high-level autonomy (Level 4) and finally complete independence (Level 5). Most clinical systems today remain at Level 1, with the surgeon controlling every motion. Yet research prototypes have already breached Level 3 territory. The Smart Tissue Autonomous Robot (STAR), for instance, has performed intestinal anastomoses on live tissue with sub-millimetre accuracy, autonomously selecting suturing paths based on real-time 3D imaging. Advances in AI are expanding the autonomy of surgical systems, although they are not yet ready to replace surgeons.
Achieving reliable autonomy in soft tissue surgery remains extraordinarily difficult. Blood, smoke, fogging, tissue elasticity, patient movement and dynamic lighting all complicate perception. Anatomical variability between patients—and even between different moments within the same operation—makes preoperative planning insufficient. Yet researchers are pushing the boundaries using reinforcement learning, imitation learning and hybrid vision-language-action models. These systems attempt to learn from thousands of demonstrations, translating complex surgical trajectories into policies that a robot can execute in real time.
Whether fully autonomous surgery is desirable remains an open question. Advocates suggest it could provide specialist care to regions lacking expert surgeons, reduce inter-surgeon variability, and maintain performance even under extreme conditions such as space travel or battlefield medicine. Critics caution that AI systems can behave unpredictably under rare or untrained conditions, and that the loss of human oversight may carry risks we do not yet fully understand. What is certain is that autonomy will not arrive all at once, but rather as an incremental layering of assistance, decision support and controlled independence..
A New Alliance Between Humans and Machines
Robotic surgery represents neither a takeover by machines nor a passing technological fad. Instead, it is the beginning of a long partnership between human judgement and mechanical precision. In this alliance, robots provide steadiness, reproducibility and computational insight, while surgeons contribute experience, intuition and ethical reasoning. Together, they can accomplish what neither could achieve alone.
Health and Social Care Secretary Wes Streeting, speaking about the NHS’s technology strategy, stated that “Innovative treatments and technologies that help fast-track better outcomes for patients is how we transform our NHS and make it fit for the future… Whether it’s robotic surgery… our Plan for Change is driving forward new ways to help cut waiting lists and get patients treated on time again.”
The future may indeed bring autonomous systems capable of performing entire procedures without human hands guiding them. But for now, the most profound change lies not in replacing surgeons but in augmenting them—giving them better tools, safer techniques and new ways of imagining what is surgically possible.
Robotics is reshaping not only how we operate, but also how we think about the boundary between human and machine. The question is not whether robots belong in the operating theatre, but how we ensure that their presence expands access, improves outcomes and strengthens—not weakens—the trust that lies at the heart of the doctor–patient relationship.


