





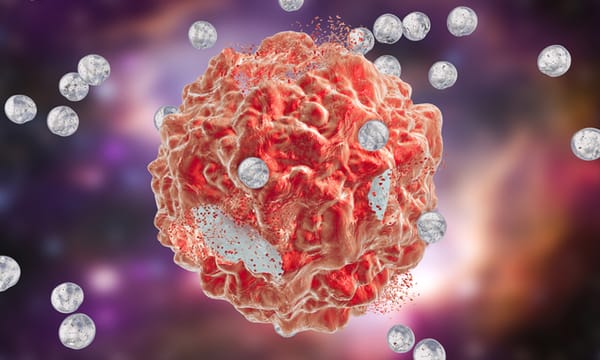

How Neuroactivating Substances Change The Brain
Rising stimulant use among young adults raises a vital question: what do these drugs really do to the brain? This article uncovers how substances like cocaine, and even caffeine, rewire emotion, motivation, and control, revealing how short-term highs can leave lasting marks on the mind.
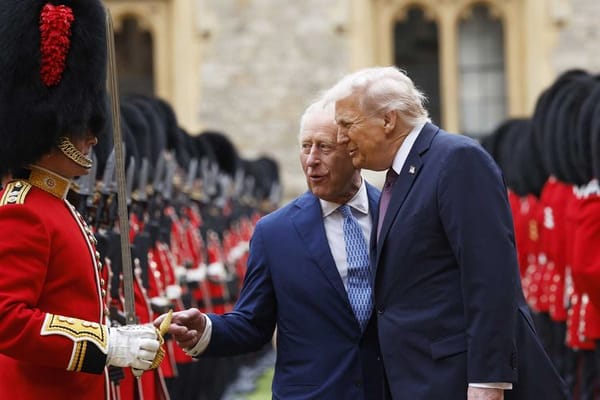
Tech Prosperity Deal: A Breakdown
The news has recently been filled with stories of Donald Trump’s 2nd state visit to the UK, the first time any US president had been invited for a second visit. Over roughly 24 hours from his arrival on the 17th of September to the morrow, he was entertained with
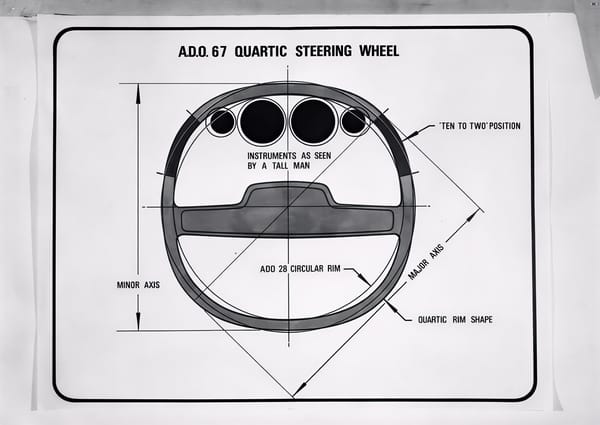
Square Wheels and Tech Traction
From flop to the top. What the once-mocked square steering wheel and electric glasses can teach us about technological innovation.

Can We Colonise Mars?
It has been pitched as everything from humanity’s ‘backup’ planet to Elon Musk’s future retirement home. For decades, the concept of humans living on Mars has been a topic of interest whether it's between space scientists, sustainability experts or even science-fiction writers. SpaceX openly talks about

The Hand-Cannon: What Was In Between Cannons and Modern Guns?
At some point during the 12th and 13th centuries, warfare and history in general were changed forever. The first cannon was invented in China, likely based on an earlier gunpowder weapon known as the fire lance. The technology spread all around the known (at the time) world. The design was

Nature’s Blueprint: How Some of Humanity’s Best Designs Come From The Natural World
In a world that is constantly seeking new and innovative solutions, scientists, engineers, and designers are turning to an unexpected source of inspiration: nature itself. Biomimicry, the practice of learning from and mimicking the strategies found in the natural world, has driven breakthroughs in everything from architecture and medicine to
Nuclear Fusion: The Power Of Future
As decades go by, the common sources of energy, like coal, fossil fuels or natural gases, are coming to extinction. While renewable power plants like wing turbines or solar panels can be used to extract energy, it won’t be enough to power the whole world. So, in order to
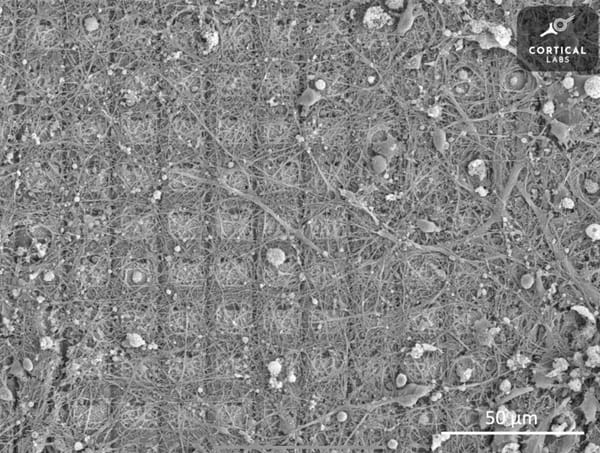
How Does ChatGPT Work?
89% of students admitted to using ChatGPT for assignments according to a study by Forbes yet most scientists who develop AI can’t fully tell you how it works. ChatGPT can write essays, generate creative works, assist in scientific research and have in-depth conversations but yet if you were to
Self-Healing Polymers
Dive into the uses, mechanisms, and chemistry behind these cutting-edge materials, and the inevitable challenges that such creations might face in practice

Mathematics in politics
Introduction Since around 500 B.C., the ancient Greek civilization introduced one of the earliest forms of democracy. Back then, voters would write their choices on broken pieces of pottery called ‘ostraka’. Imagine a world where the outcome of a major election isn’t just about the number of people

Stay Curious, Be Adaptable: A Profile of Sanjay Patel OE
Sanjay Patel and his wife Leslie were involved in the rebuilding of a wind tunnel. That I couldn’t grab a second to ask why indicates the pace of a Sanjay Patel conversation. He’s a whirlwind of insight, brilliance and empathy, his thoughts speeding far ahead of one’s

Relief Channels and Re-Meandering to Mitigate Flooding
Floods can devastate cities, but what if we fought water with nature instead of just concrete? While relief channels redirect raging rivers, a quieter revolution is unfolding: re-meandering rivers to slow floods, restore ecosystems, and rethink how we shape the land.